
How It Works
Discover what measurements the Citec can aid you in.
Click the muscle groups highlighted below.
How It Works
Discover what measurements the Citec can aid you in.
Click the muscle groups highlighted below.
Neck extensors
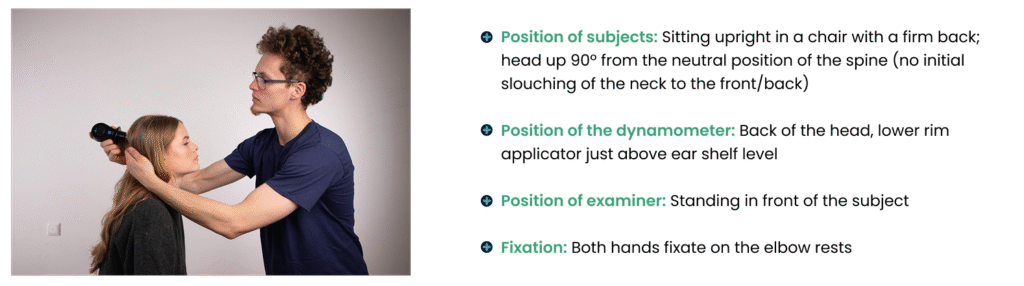
Additional remarks
Watch out for compensating muscle activation – measure only Neck muscles!
Some subjects experience pain in their neck extensors, which will influence MCV (Maximum Voluntary Contraction) and reliability.
The tendency of the subject to elongate these muscles by bending the trunk backwards is prevented by the chair. In the described examiner position, it is not possible to measure beyond +/- 125N. Most normal subjects are stronger than this value. For males, a value <125N must be regarded as subnormal.
Neck flexors
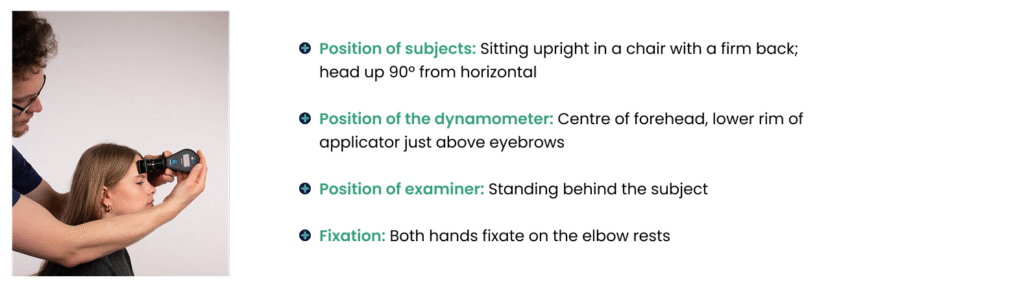
Additional remarks
Some subjects experience pain in their neck flexors, which will influence MCV (Maximum Voluntary Contraction) and reliability. Not infrequently, pain is caused by the pressure of the dynamometer on the forehead. This difficulty can be removed by a small soft pad between the applicator and the forehand.
The subject will have a natural tendency to elongate these muscles by bending the trunk forward, which cannot be prevented totally, but a fast movement must be avoided, because this will result in a fast eccentric contraction and a higher value.
Shoulder abductors
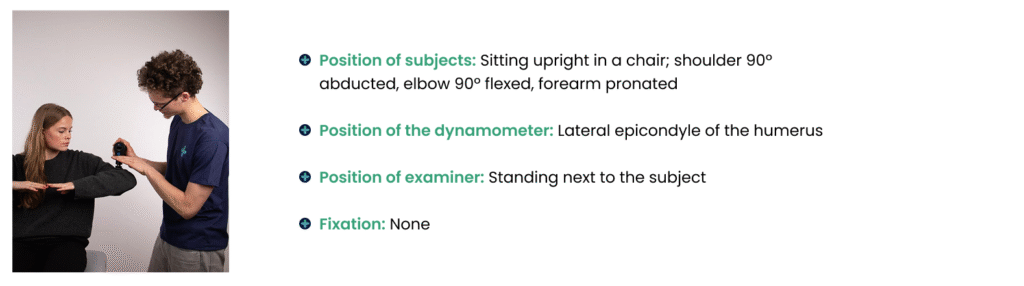
Additional remarks
For good symmetry, it is advised to bring both arms to the position described. Bending to the contralateral side must be avoided. This elongates the deltoid muscle and will influence the result.
In this position, gravity has a marked influence. In subjects with severe weakness in these muscles, an alternative would be a supine position with otherwise the same standardisation.
Shoulder abductors
Additional remarks
For good symmetry, it is advised to bring both arms to the position described. Bending to the contralateral side must be avoided. This elongates the deltoid muscle and will influence the result.
In this position, gravity has a marked influence. In subjects with severe weakness in these muscles, an alternative would be a supine position with otherwise the same standardisation.
Elbow flexors
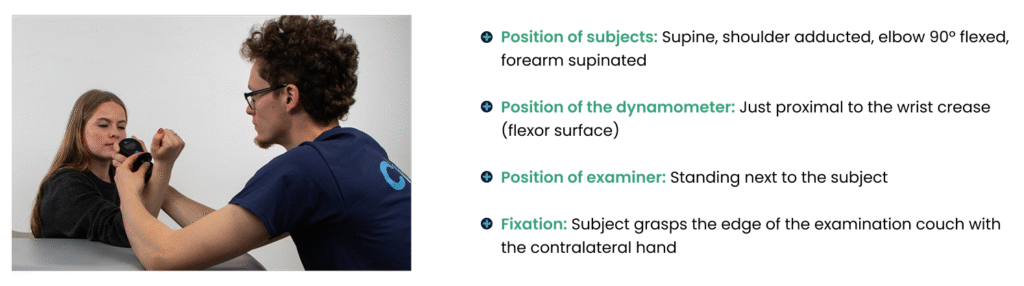
Additional remarks
The subject must lie down flat with at most one cushion, otherwise the standard position will be inferred. There is a tendency to move the shoulder up and forward, elongating the bi-articular biceps muscle.
Especially the male elbow flexors can be very strong. Above 200N, it is often necessary for the examiner to sit directly against the supinated forearm to give additional support to prevent pulling the subject from the examination couch. It is impossible to measure both elbow flexors from one side.
Elbow extensors
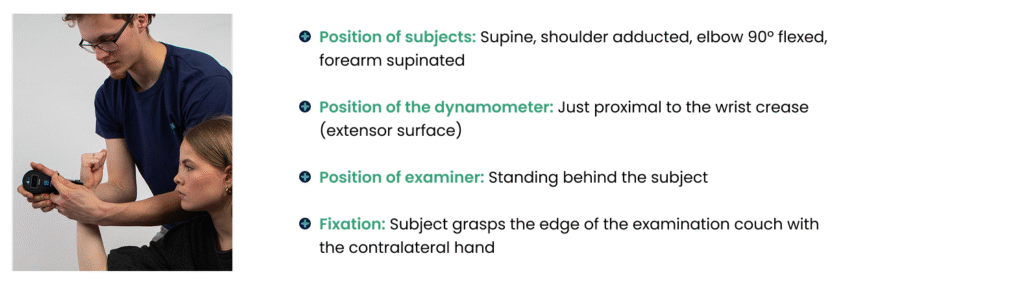
Additional remarks
The subject must lie flat with at most one cushion, otherwise the standard position will be inferred. Many subjects have a tendency to raise their elbows, but with proper instructions, this can be prevented.
Wrist extensors
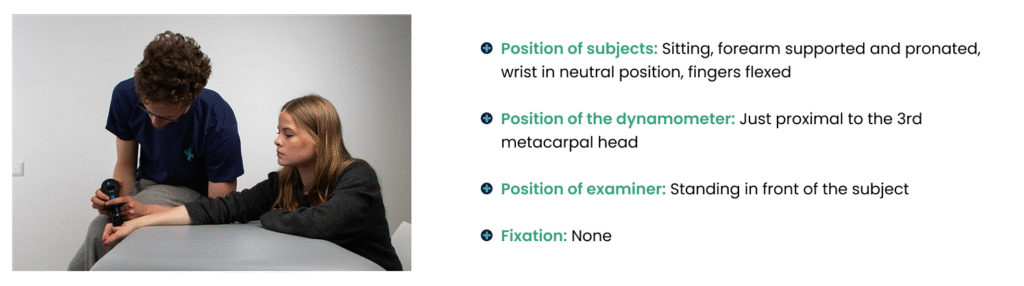
Additional remarks
The participant is seated next to the test table with the shoulder positioned at approximately 30° abduction, the elbow flexed to 90°, and the forearm in a neutral position. The forearm is stabilized on the table, for example using four fixation pegs, to prevent compensatory movement during the test. The wrist joint is placed at the edge of the table, with the wrist and fingers maintained in a neutral position.
To avoid discomfort, the table edge should not press sharply into the wrist. If needed, one or two folded tissues can be placed under the wrist joint. Similarly, the contact area of the dynamometer should be checked carefully, as pressure is applied over the distal metacarpals.
The hand-held dynamometer is fixed to the test table, with its contact point positioned on the distal metacarpal region. The measurement is performed using the make method, in which the participant gradually increases force against the fixed dynamometer. The examiner may stabilize or hold the dynamometer with both hands and increase counterforce slowly by leaning with their own body weight. Force application should be gradual and controlled, taking approximately 1–2 seconds, rather than sudden or brisk.
This gradual procedure is especially important for the wrist extensors, because a rapid break test can produce an artificially high strength value and should therefore be avoided. Although gravity acts on the wrist in this position, it has no practical influence on the measurement. If the wrist extensors are too weak to overcome gravity, approximately 2–3 N, the generated force would still be too small to produce a readable value on the dynamometer scale
Three-point grip
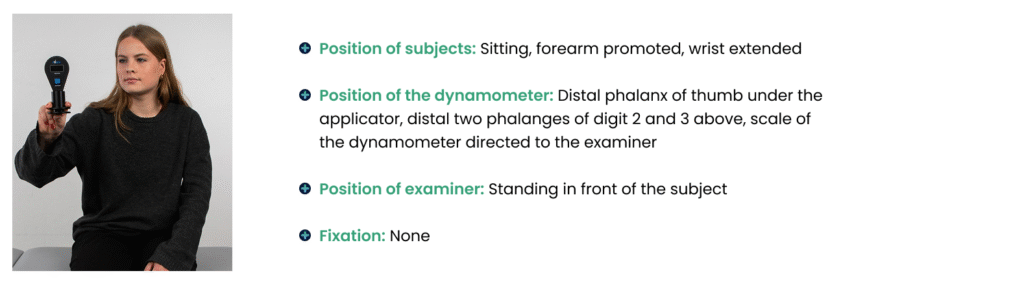
Additional remarks
This is the only test in which the contraction is truly isometric. The examiner must prevent the 4th and 5th finger are compressing the dynamometer too. Prevention is easily possible by bending these two fingers before the contraction.
Hip abductors
Additional remarks
The right and left hip abductors are difficult to measure separately because, for stabilisation of the pelvis, the contralateral abductors must contract too. Therefore, both sides are tested at the same time, and the weakest side will determine the result. This drawback is not serious, because weakness of these muscles seldom occurs unilaterally, but nearly always bilaterally and symmetrically, as in proximal myopathies.
Hip flexors
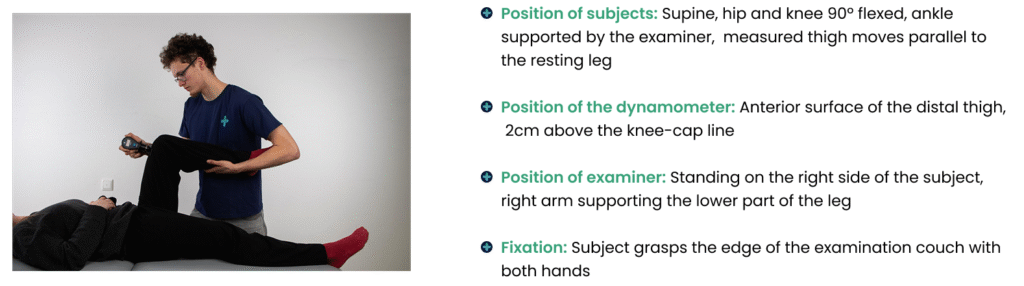
Additional remarks
Some synergistic hip flexor muscles are bi-articular (rectus femoris, tensor fasciae latae and sartorius), and the subject will try to elongate these muscles by bending the knee. Supporting the lower part of the leg counteracts this unwanted movement effectively.
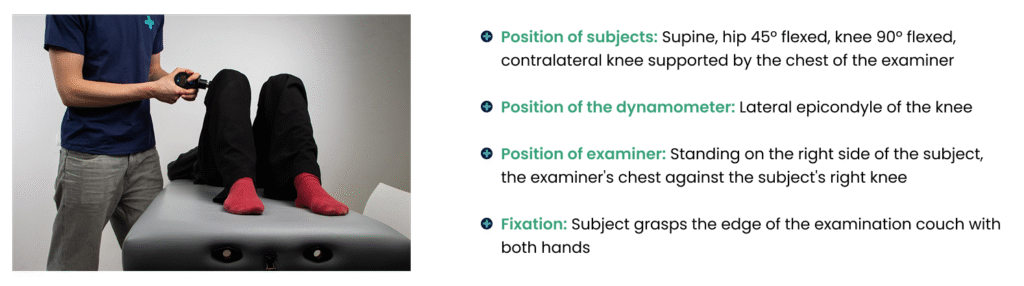
Knee extensors
Additional remarks
The standard and well-validated position for measuring knee extensor strength with a hand-held dynamometer is seated, with the hip and knee flexed at 90°. The dynamometer should be positioned at the ankle, approximately 2 cm above the malleoli. The patient pushes against the dynamometer in a controlled manner.
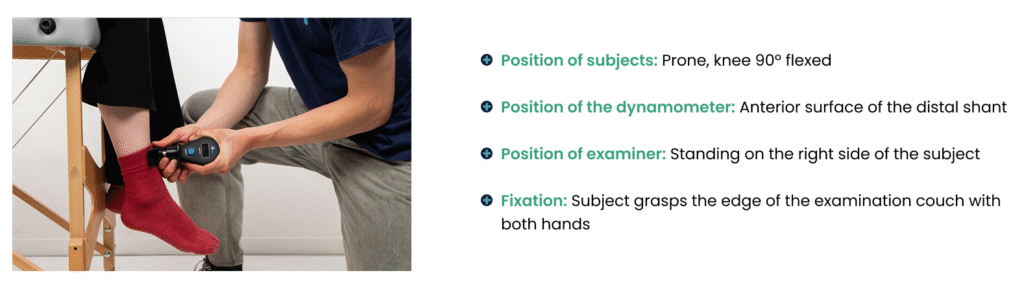
Knee flexors
Additional remarks
Because all hip flexors are bi-articular, there is a strong tendency to elongate these muscles by raising the buttocks. Even with clear instructions, it is hard to suppress, and without doubt, it will influence the result. A belt over the posterior pelvis could help, but this would be time-consuming, and the test-retest results in normals would not be much worse compared with other muscle groups. A large part of healthy subjects develop cramps during the contraction. Formerly, we measured with a knee flexed 90º, and in that position, cramps occurred even more often, hindering correct strength assessment. It is clear that cramp will negatively influence the strength level and the reliability of the results.
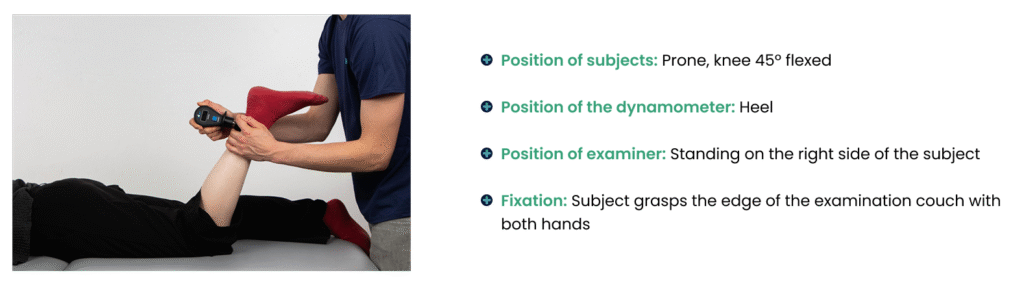
Foot dorsiflexors
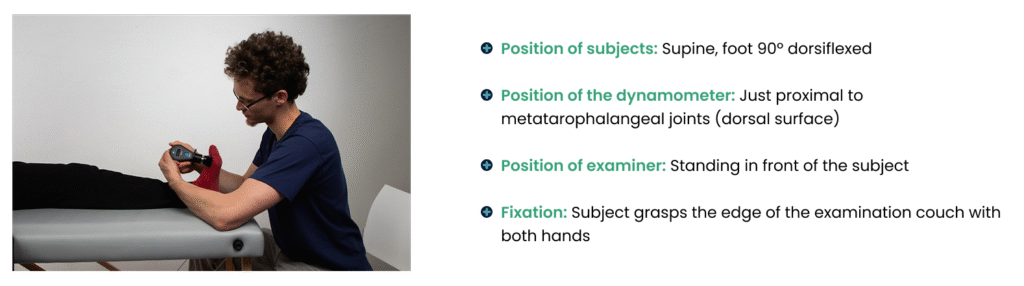
Additional remarks
This muscle group is not easy to measure. It is difficult to determine at which moment the muscle gives away. Giving away of these muscles consists of a minor displacement of the foot, but with careful inspection, this slight movement can be perceived.
Foot plantarflexors
Additional remarks
Ankle plantar flexion is commonly tested in the supine position; however, this measurement has important limitations. At higher force levels, reliability may be reduced because the examiner may not be able to stabilise the hand-held dynamometer effectively against the strong force produced by the plantar flexors. Therefore, this test is mainly suitable for individuals with marked or severe plantar flexor weakness. In stronger individuals, the results should be interpreted with caution, as they may reflect limitations of the testing method rather than true muscle strength. Additionally, in subjects with severe paresis, plantar flexor contracture may prevent testing in the standard 90° dorsiflexion position, making it difficult to distinguish between voluntary contraction and passive muscle stretch.